Pathology
Achondroplasia occurs during ossification of the bones. Ossification occurs in two parts; intramembranous ossification which involves the bones of the skull vault, the face and the clavicle, and endochondral ossification which involves all remaining bones (Manchester et al. 1995). With achondroplasia, there is an inhibition of cartilage formation, thus preventing normal endochondral ossification . The bones that have the fastest growth and the least number of growth plates are the most affected. Therefore, the trunk is of relatively normal size because of the large amount of growth plates in the spine, while the long bones, which have only two growth plates, are not. The most shortened bones of the body are the femur, the humerus, and the bones of the forearm and lower legs (Ortner et al. 1981). Often, the bones of the arm are so shortened that the fingers reach only to the hips (“Achondroplasia” n.d.).
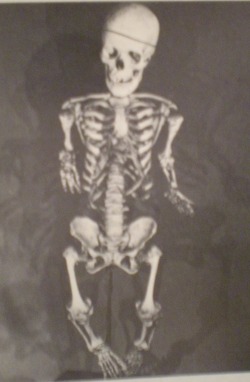
Figure 2 (Ortner et al. 1981: 330): Achondroplastic adult female dwarf with noticeably short and thick long bones.

Other than shorter than normal stature, achondroplastic dwarfs often have thick long bones relative to their length. They often display a bulging forehead, a short skull base, a small face and a depressed nose bridge, protruding jaw, short, broad hands, bowed legs, prominent buttocks and small chests (Brothwell 1981). Although the small proportions of the body make the skull appear large, occasionally the increased size can be due to hydrocephalus; in this case, surgery would be required ("Achondroplasia: Fact Sheet" n.d.). Many of those with this condition can only extend the elbow joint to 150 degrees. Common spinal curve defects include severe lumbar lordosis, or inward curvature of the lumbar, and thoracic kyphosis, or a concave curvature of the thoracic area of the spine. Also, the pelvis is narrow, especially between the pubic symphysis and the sacral promontory, which can cause achondroplastic women difficulty during childbirth (Ortner et al. 1981).
Although adult dwarfs often show accentuated muscle insertions, achondroplastic infants are sometimes found to have lower muscle tone than infants without the condition. This is due to the fact that achondroplatic dwarfs do not begin to walk until 24 to 36 months. Because of the short stature of dwarfs, obesity often occurs. Also, the abnormal size and structure of the skull and jaw can lead to malocclusion and an overcrowding of the teeth ("Achondroplasia" n.d.)
Figure 3 (Dasen 1993: 355): Typical achondroplastic boy
Figure 4 (Ortner et al. 1981: 330): Narrow achondroplastic pelvis with short femora and accentuated muscle insertions.
Figure 5 (Filer 1996: 57): An achondroplastic right femur and a normally sized left femur


